Women's Fertility Biomarkers Explained
Fertility isn't binary — it exists on a spectrum influenced by hormonal balance, ovarian reserve, thyroid function, and other measurable biomarkers that shift with age, nutrition, and lifestyle. Understanding where you stand right now gives you information to work with, whether you're actively trying to conceive, planning ahead, or simply curious about your reproductive health.
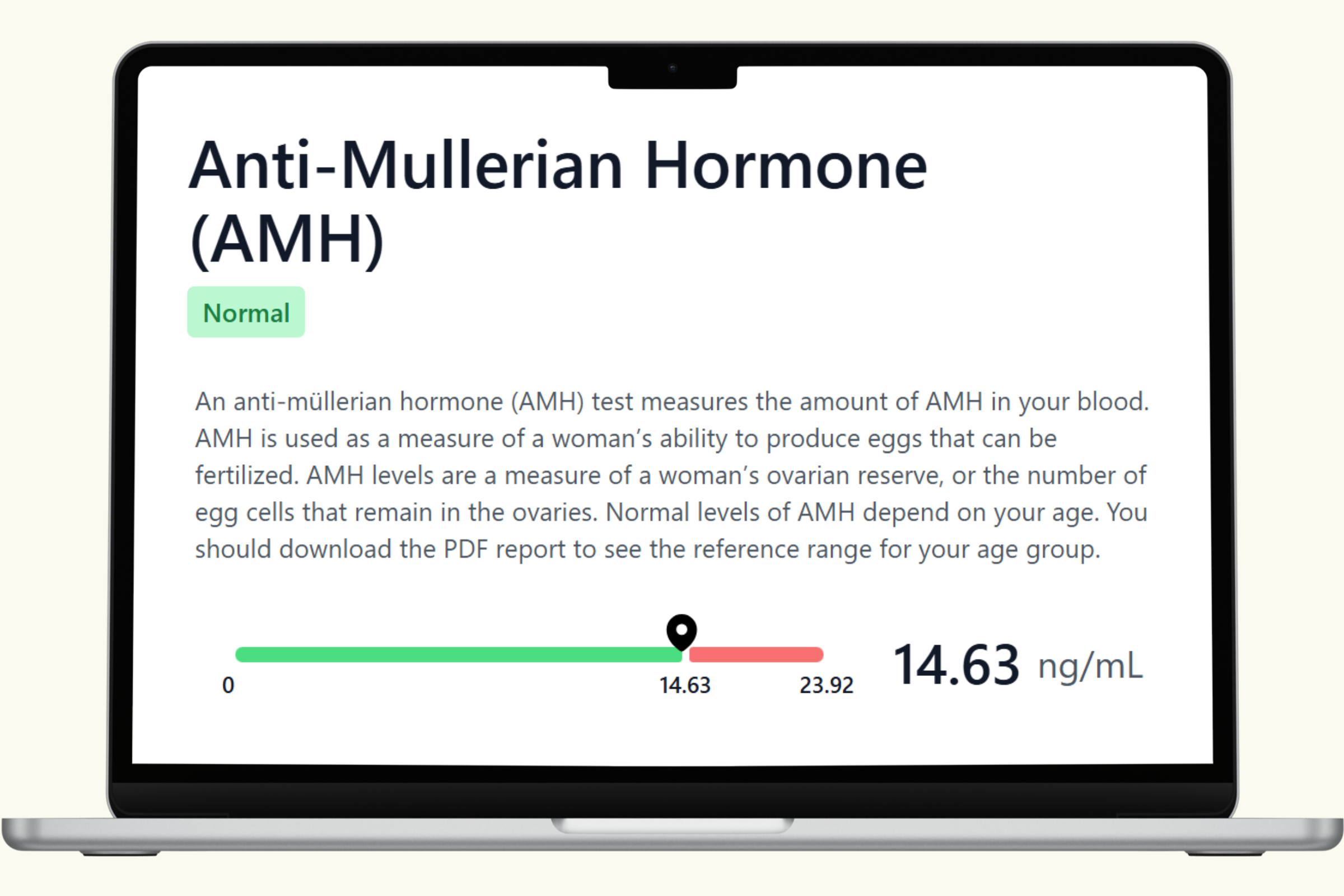
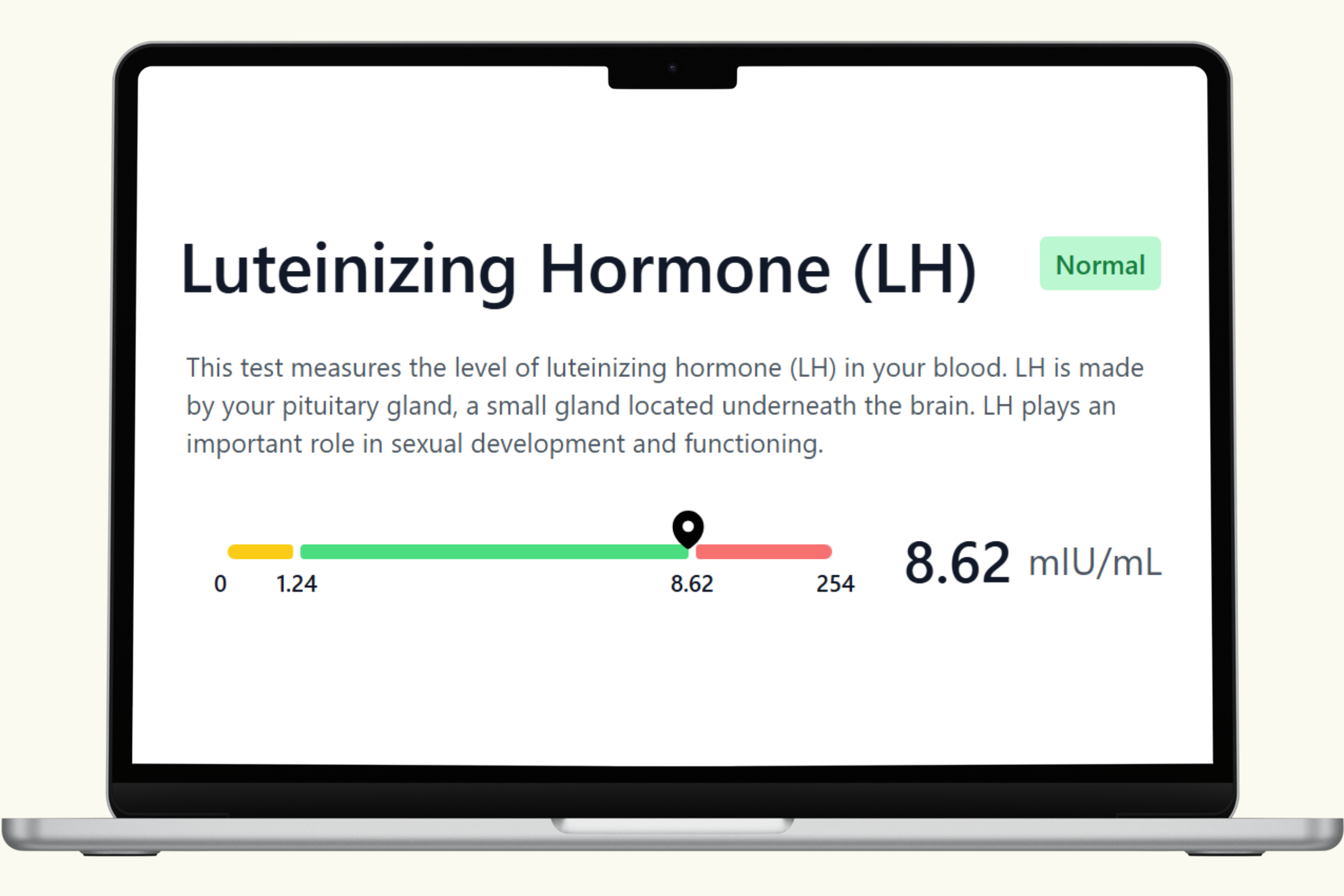
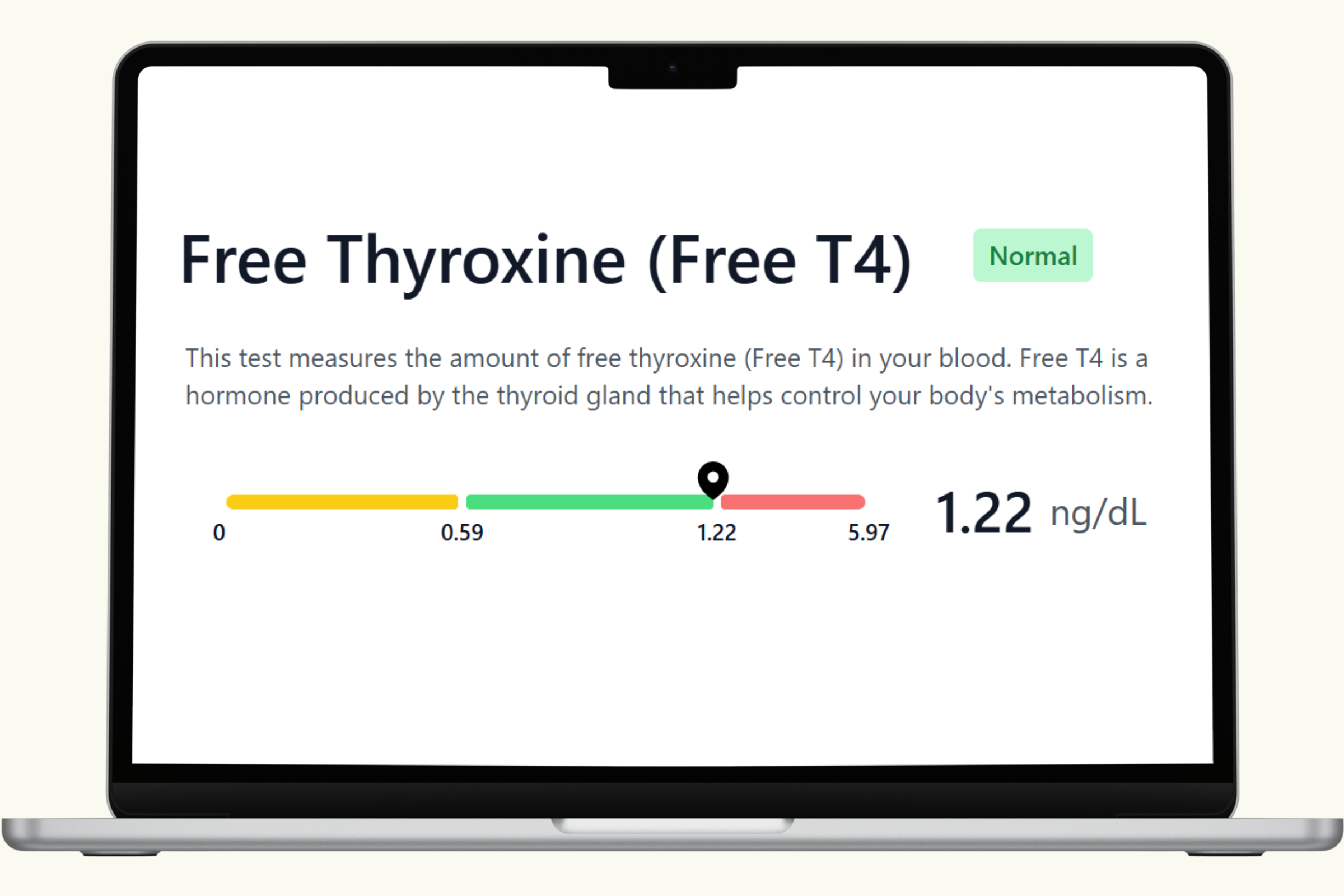
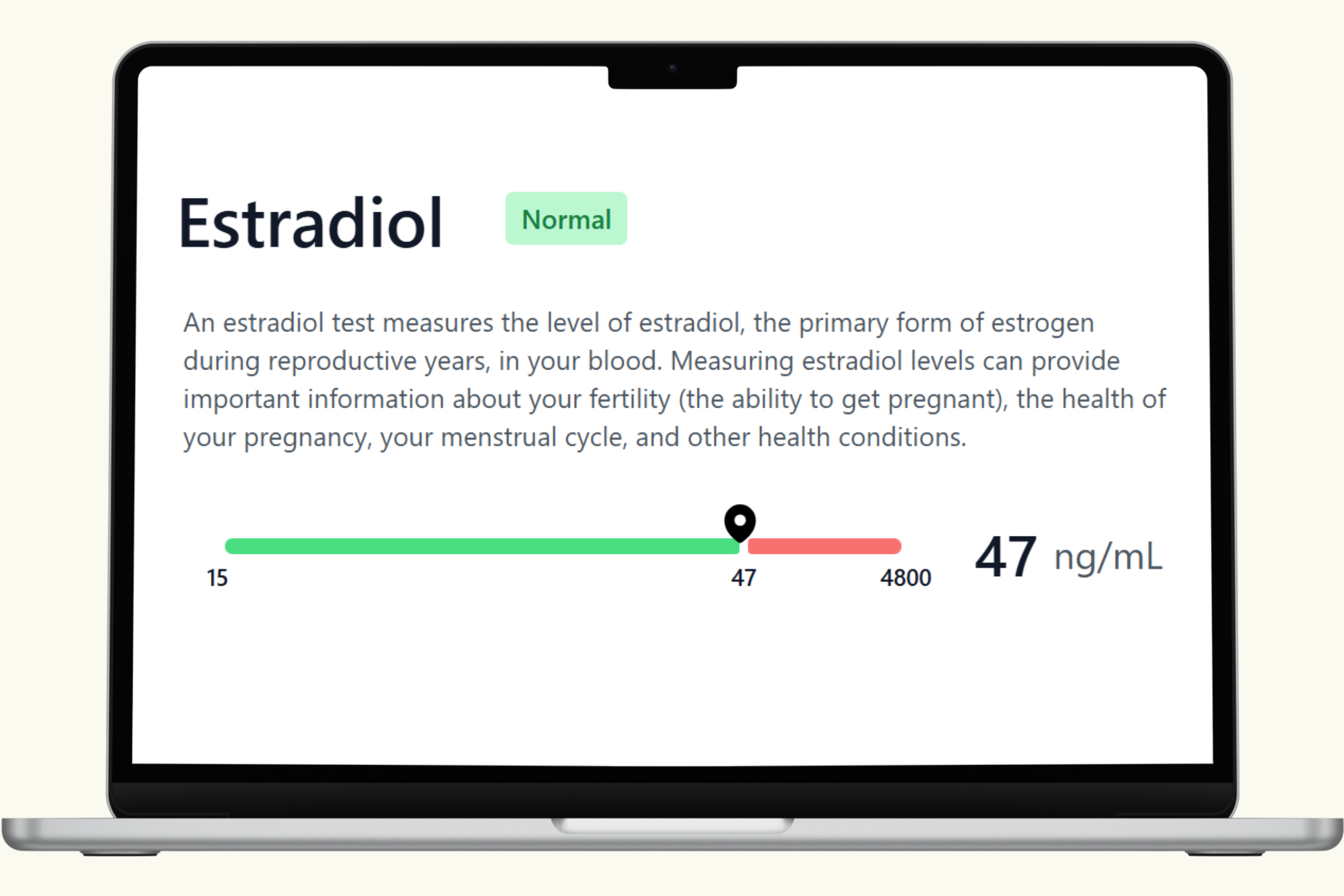
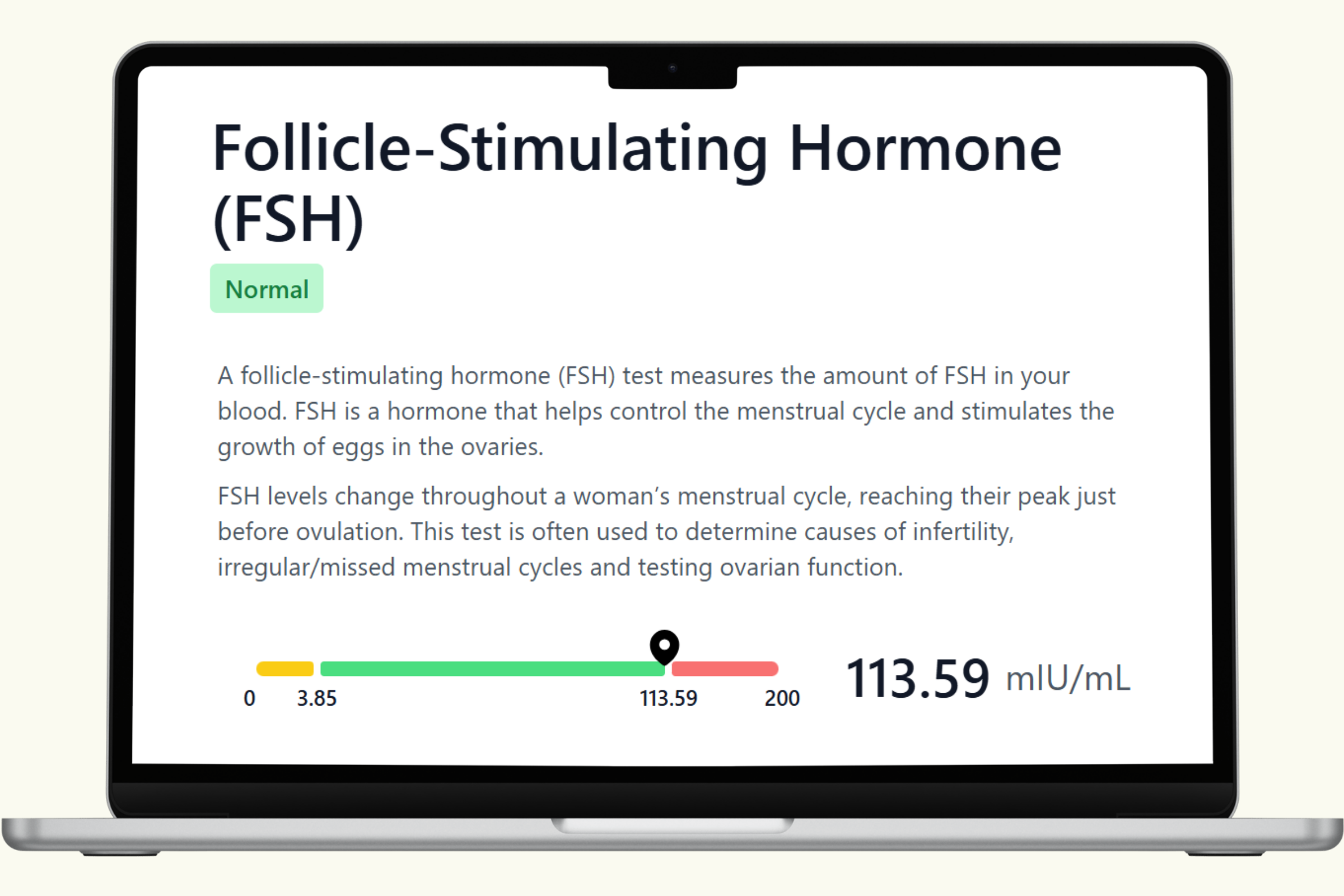
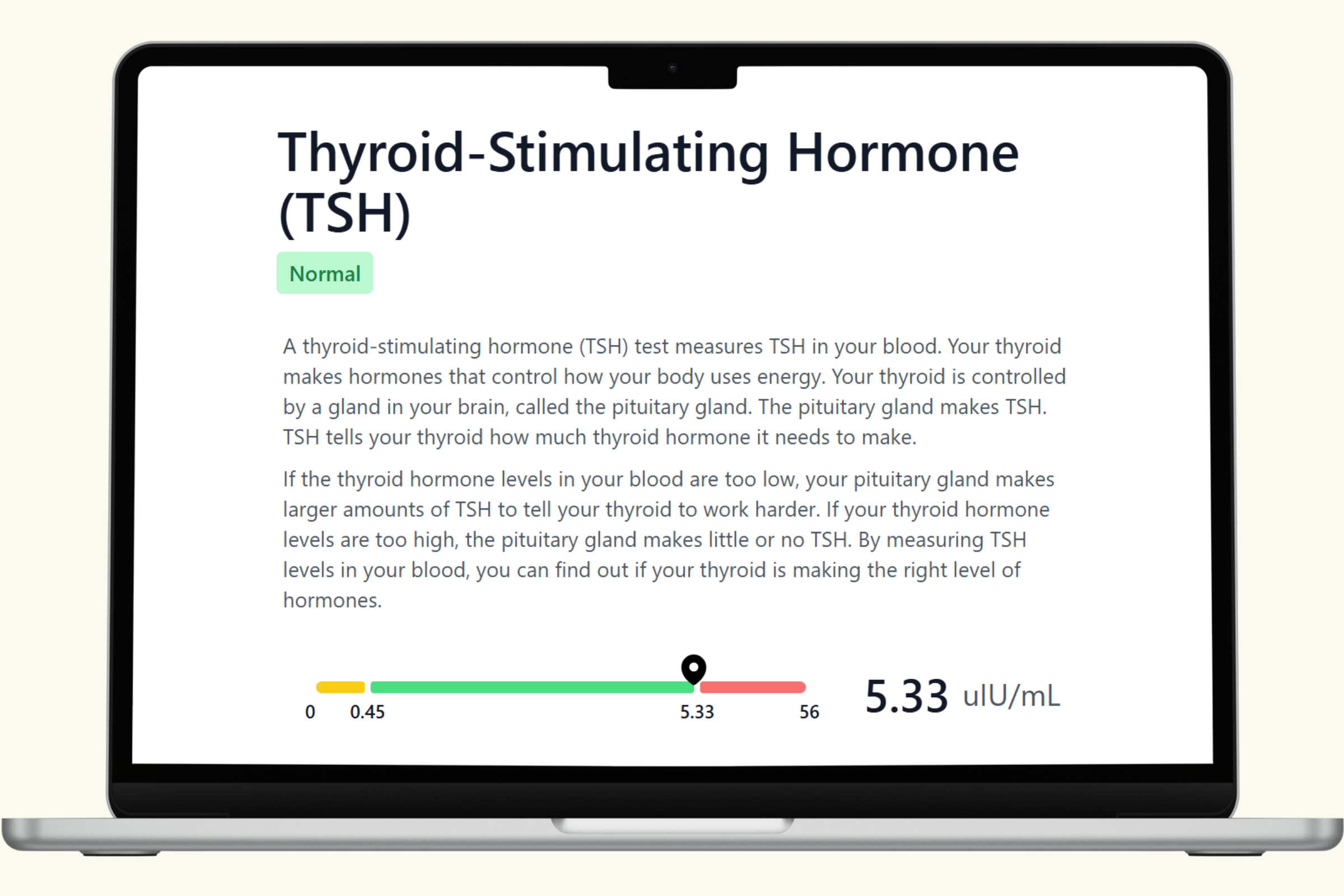
This hub covers each biomarker in the PlexusDx Women's Fertility Blood Test — what it measures, what influences it, and how it connects to the hormonal systems that support reproductive health. Results are delivered through your Results Portal within 5 business days (hormone panels require additional processing time) with personalized guidance.
For a complete picture, many customers pair fertility blood results with the Precision Hormone & Reproductive Health Genetic Test to understand both current hormonal status and long-term genetic tendencies.
No doctor's order required. HSA/FSA eligible.