Men's Hormone Biomarkers Explained
Testosterone, DHEA-S, and related hormonal biomarkers influence far more than most men realize — affecting energy, body composition, mood, cognitive function, libido, and cardiovascular health. Measuring your current hormonal status gives you real data to work with rather than guessing based on symptoms alone.
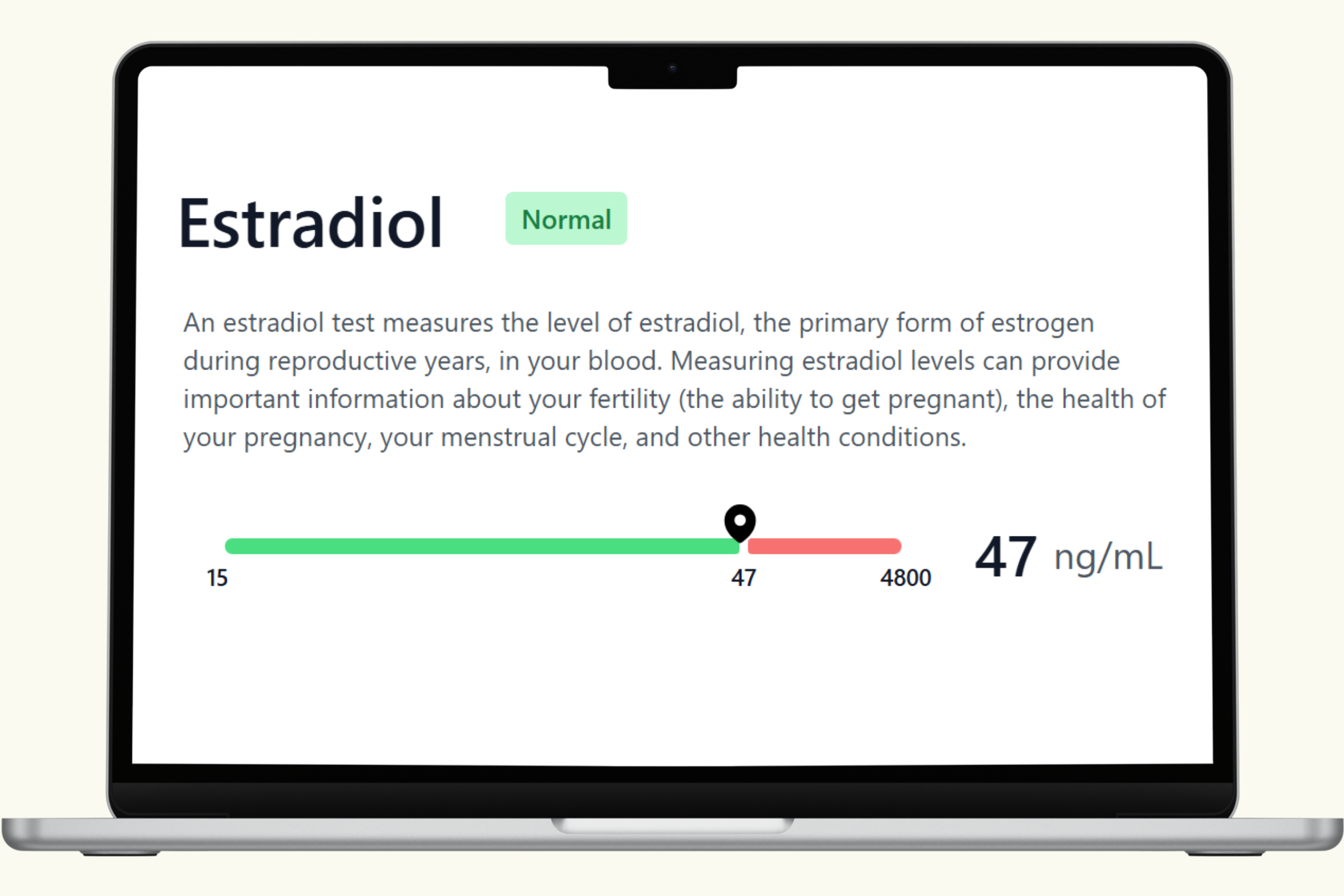
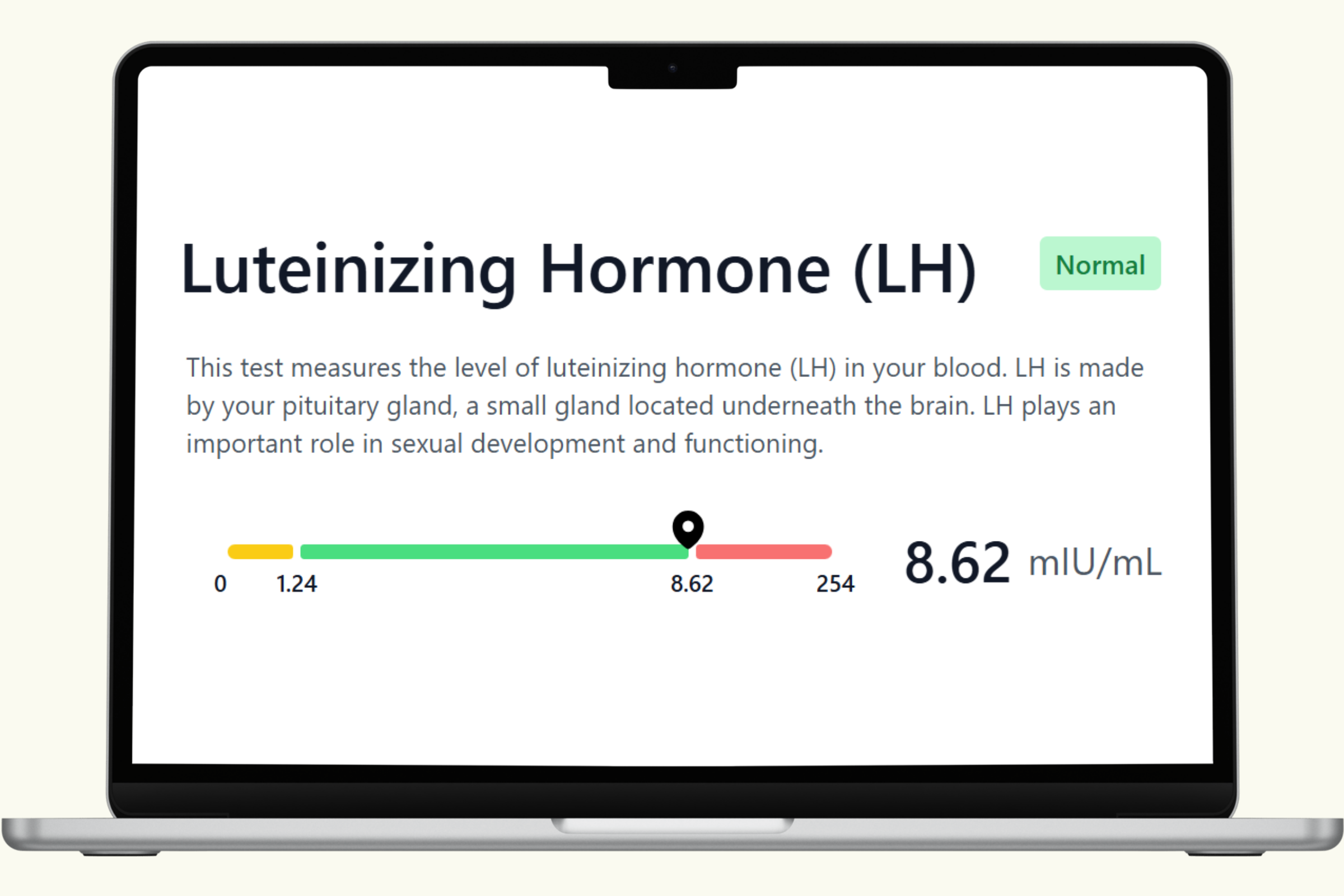
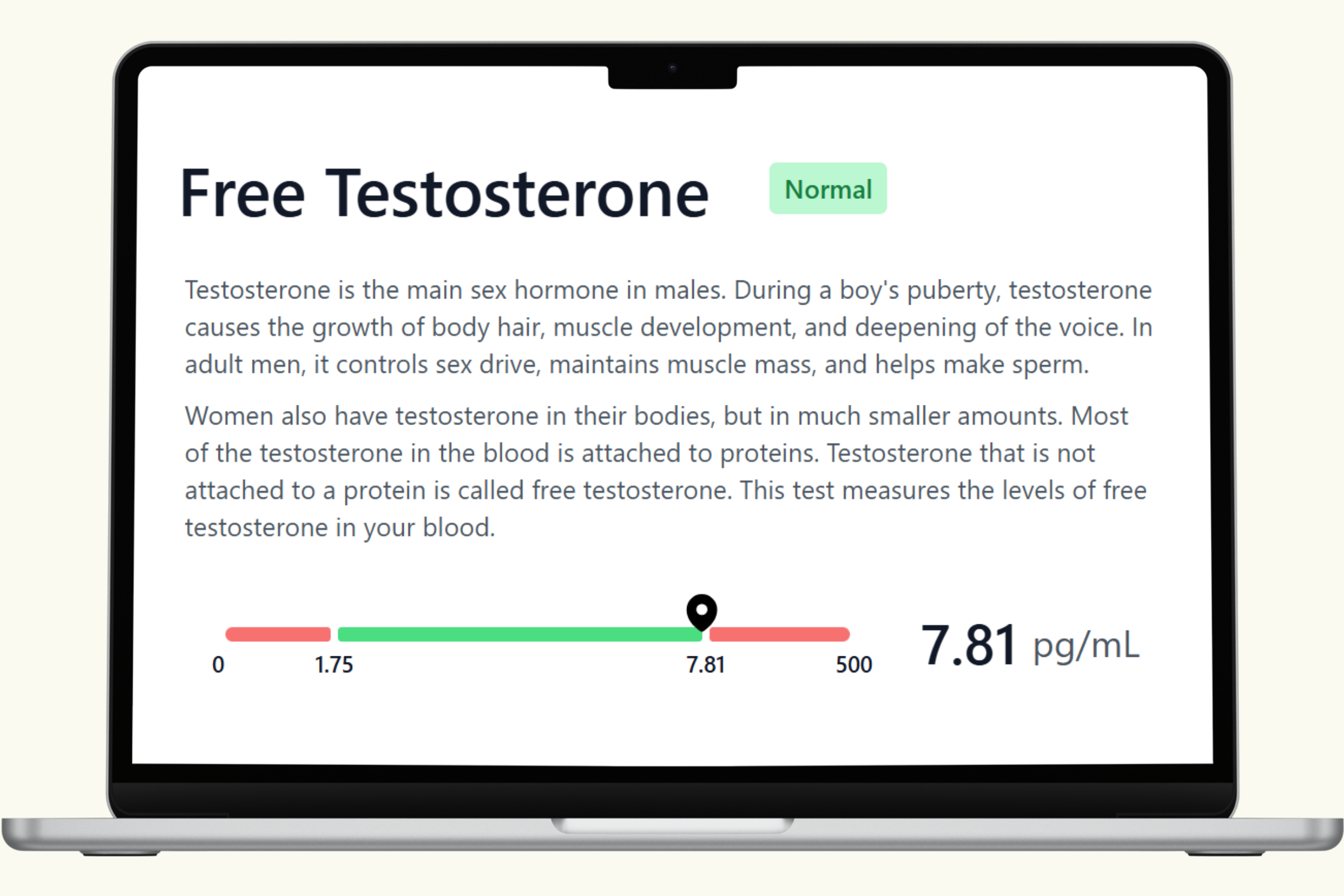
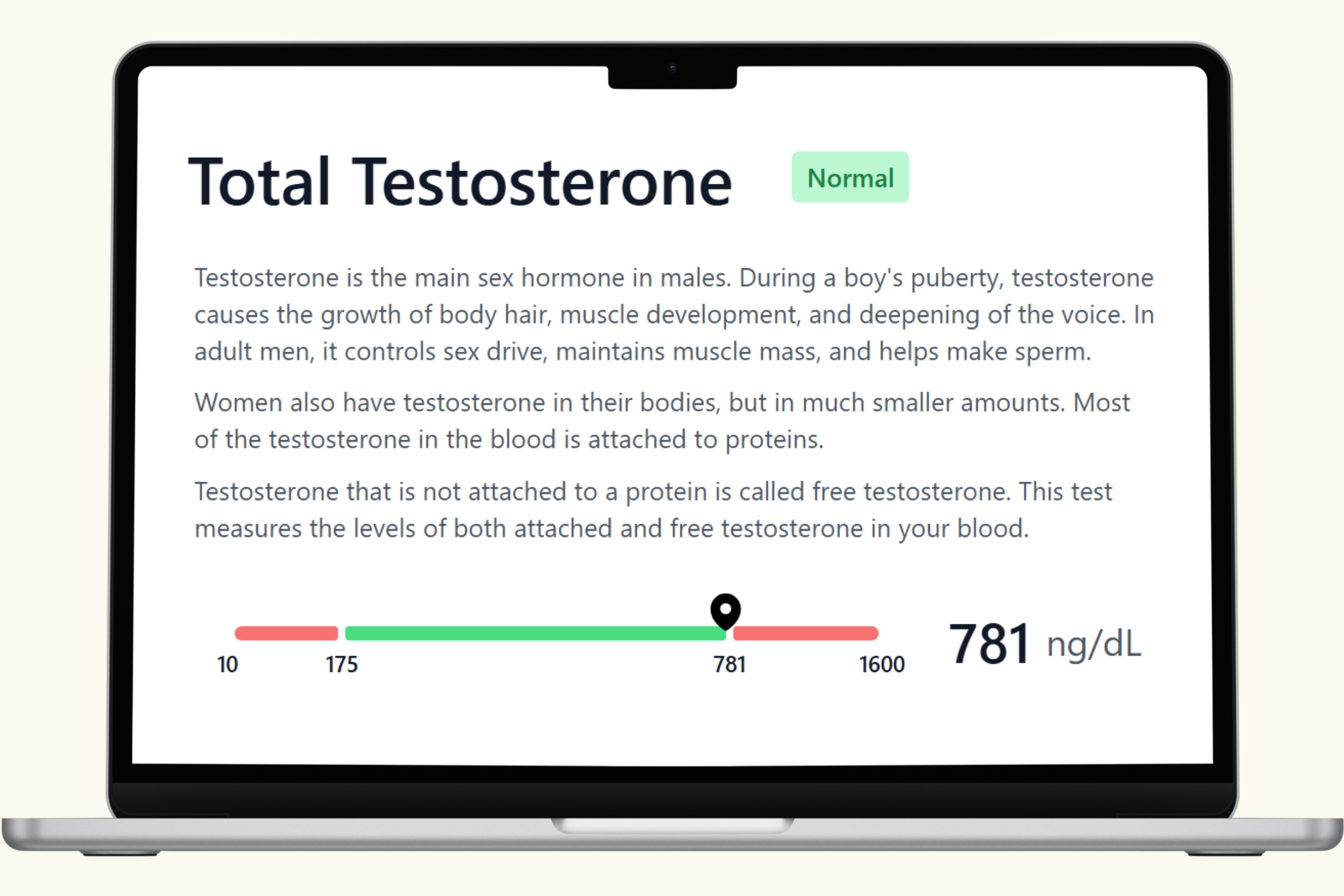
This hub covers each biomarker in the PlexusDx Men's Hormone Blood Test — what it measures, what drives it up or down, and how it connects to your overall hormonal health. Results are delivered through your Results Portal within 5 business days with personalized guidance.
For a more complete picture, many customers pair hormone blood results with the Precision Hormone & Reproductive Health Genetic Test to see both current levels and long-term genetic tendencies together in the same Results Portal.
No doctor's order required. HSA/FSA eligible.