Methylation Blood Biomarkers Explained
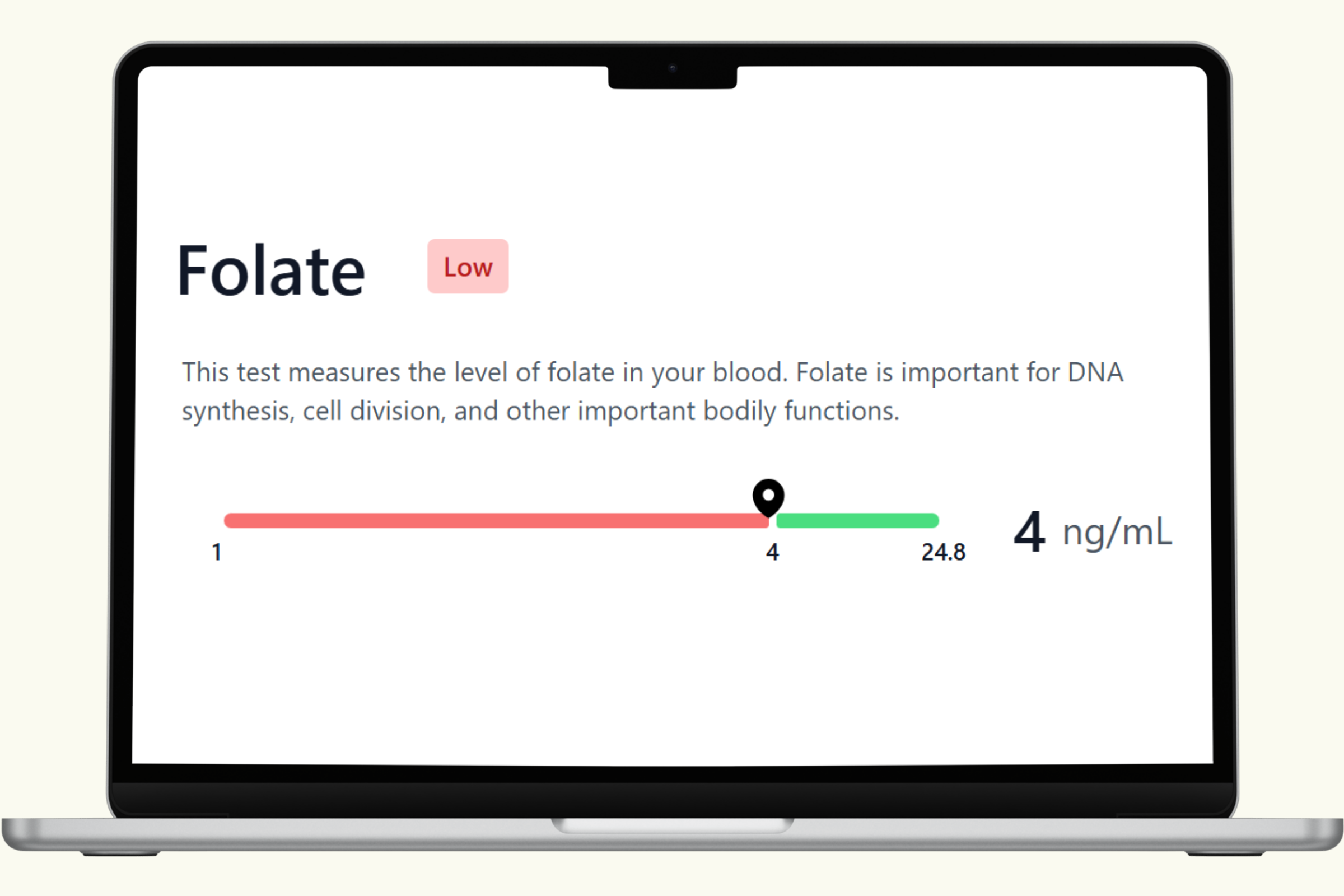
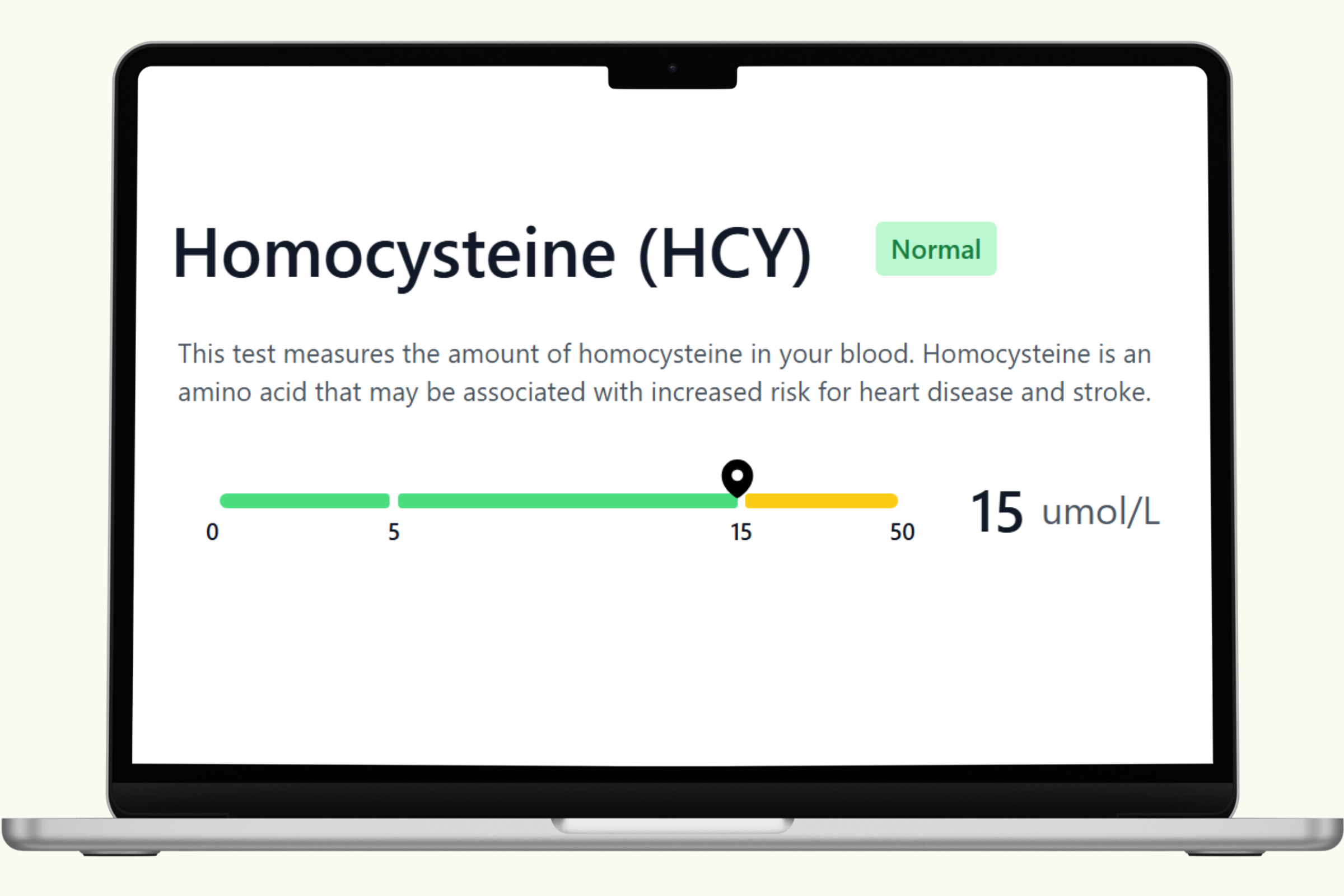
Methylation is a biochemical process your body runs continuously — governing DNA repair, neurotransmitter balance, detoxification, and cardiovascular health. Three blood biomarkers give you a direct window into how well your methylation system is functioning right now: homocysteine (a key methylation byproduct tied to cardiovascular risk when elevated), folate (vitamin B9, essential for the folate cycle), and vitamin B12 (a critical methyl donor and cofactor).
This hub covers each biomarker in detail — what it measures, what influences it, what optimal levels look like, and how it connects to the broader methylation system. Results from the PlexusDx Methylation Panel Blood Test are delivered through your Results Portal within 1–2 business days, with personalized diet and supplement guidance based on your levels.
For a complete methylation picture, many customers pair this blood test with the Genetic Methylation Test to combine current biomarker status with long-term genetic tendencies.
No doctor's order required. HSA/FSA eligible.